



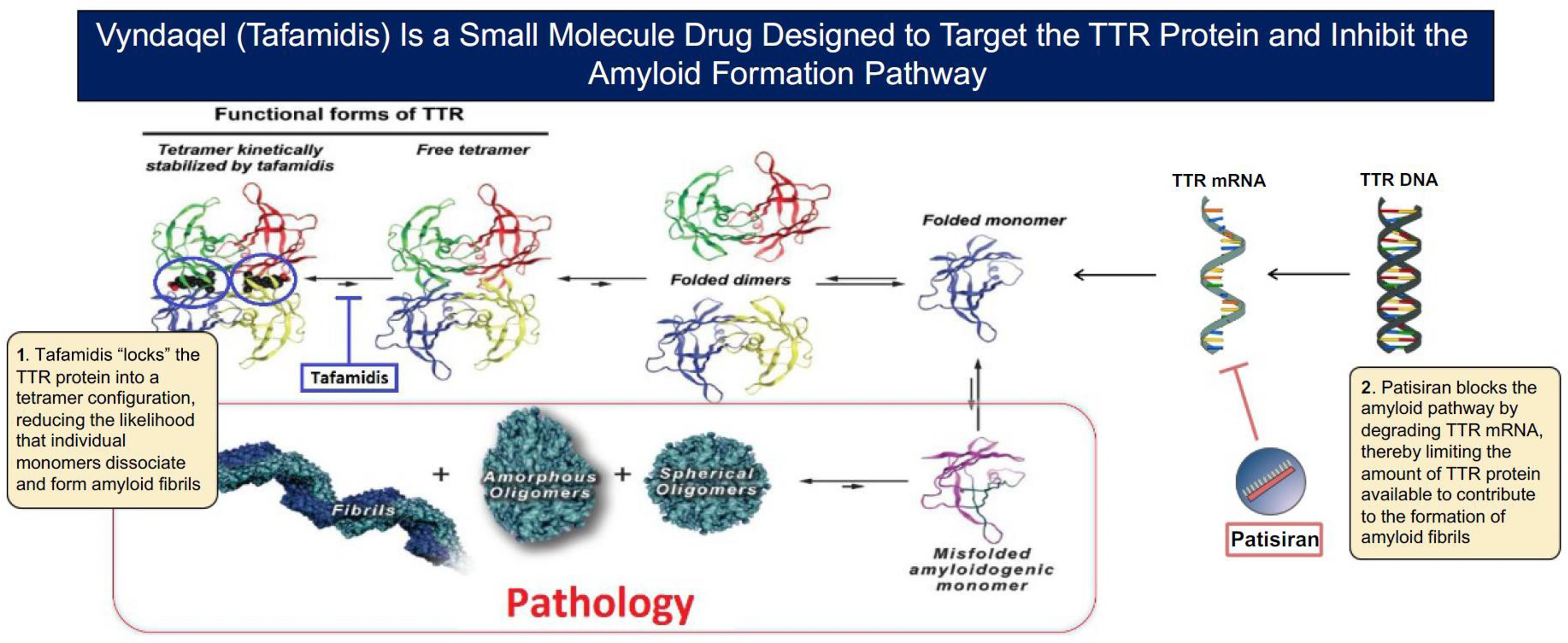
- Small molecule TTR stabilizers: provide kinetic stabilization of TTR tetramer and inhibit the initiation of amyloid formation by preventing dissociation of the TTR tetramer into monomers; preventing TTR tetramer dissociation results in slowing progression of disease and preservation of function, which is expected to translate to improved quality of life.
- TTR knockdown / RNA silencing therapies: inhibit the synthesis of TTR by the liver, thereby reducing the amount of circulating tetrameric TTR and concentration of TTR monomers available for formation of amyloid deposits.
- ALXN: Eidos DSRF Oct 2019.
Overview of Amyloidosis Supportive Care Tx Options
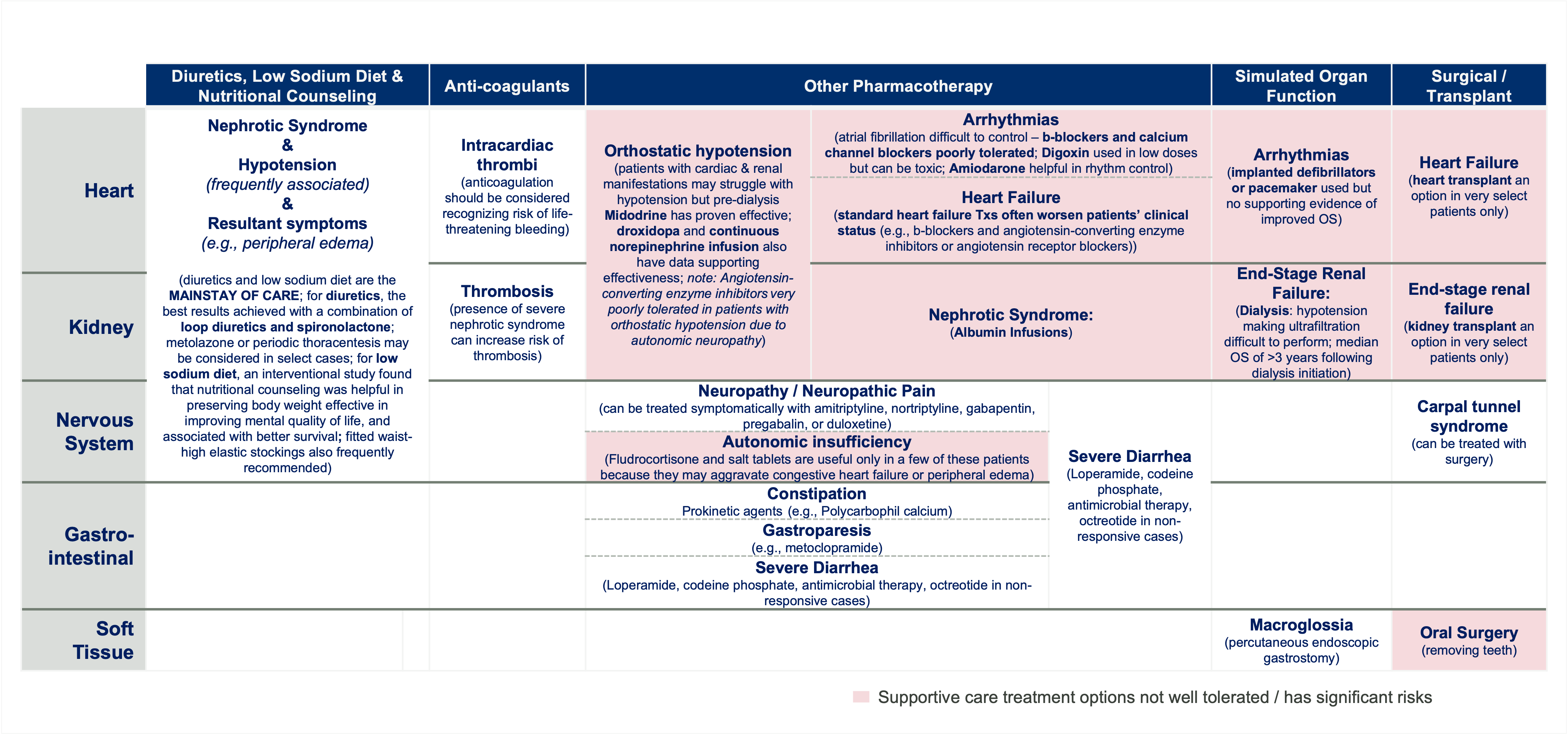
Low Sodium Diet & Nutritional Counseling:
- Malnutrition at diagnosis has been shown to predict mortality in patients with AL amyloidosis independently of cardiac stage and response to treatment8
- Peripheral edema: Patients should be frequently consulted on a low-salt diet and they should weigh themselves daily7
- Nephrotic Syndrome7: Interventional study run at our center documented that in outpatients with AL amyloidosis, nutritional counseling was helpful in preserving body weight effective in improving mental quality of life, and associated with better survival8
Diuretics:
- Diuretics are the mainstay of care, with the best results achieved with a combination of loop diuretics and spironolactone. Thiazide diuretics have less of a natriuretic effect than the loop diuretics, but are sometimes used in conjunction with them to increase natriuresis. Metolazone could be considered in patients with or without renal failure, with careful monitoring for possible hypotension9
- For patients with nervous system involvement or nephrotic syndrome, achieving a balance between heart failure and intravascular volume depletion is particularly important5
- Diuretic resistance is common in patients with severe nephrotic syndrome, and metolazone or spironolactone may be required in conjunction with loop diuretics5
- In patients with renal involvement, which is nephrotic syndrome in most, the major problem is third space fluid distribution due to hypoalbuminemia. This may be further exacerbated by coexisting cardiomyopathy17
CARDIAC:
Anti-coagulants:
- Intracardiac thrombi
- Patients with cardiac amyloid are at risk for intracardiac thrombi - 35% of patients with AL amyloidosis who had transesophageal echocardiograms had atrial thrombi19
- Anti-coagulation should be considered, recognizing that life-threatening bleeding is a potential risk17
Arrhythmias:
- For patients with atrial fibrillation, rate control can be a challenge because b-blockade and calcium channel blockers are often poorly tolerated. Digoxin has been considered contraindicated in cardiac amyloidosis due to concerns regarding digoxin binding and an increased risk of toxic effects but digoxin is often preferred over calcium channel blockers and b-blockers for rate control in atrial fibrillation17
- Recent data indicates it can be tolerable at lower doses while frequently monitoring drug concentration and closely monitoring electrolytes and kidney function14
- Amiodarone is often helpful for rhythm control17
Positive:
- Midodrine1
- Renal patients undergoing dialysis may struggle with hypotension, which can be successfully managed with predialysis midodrine17
- Continuous norepinephrine infusion5
- Reported to be a successful treatment of severe hypotension that is refractory to conventional treatment5
- Droxidopa1
Negative:
- Angiotensin-converting enzyme inhibitors1
- Afterload reduction with angiotensin-converting enzyme inhibitors or angiotensin receptor blockers also tends to be poorly tolerated in patients with cardiac AL amyloidosis, especially in those who have orthostatic hypotension due to autonomic neuropathy17
Heart Failure
- The use of standard medical therapy for heart failure with reduced ejection fraction, specifically, b-blockers and angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, often worsen patients’ clinical status17
- Patients with reduced stroke volume can benefit from afterload reduction with angiotensin- converting enzyme inhibitors6 However, these agents should be used cautiously, starting with a low dosage and withdrawing if postural hypotension develops6
- B-blockade cause profound hypotension and low cardiac output and should be avoided17
- Calcium channel blockers can aggravate congestive heart failure in amyloid cardiomyopathy and generally should be avoided5
Notes: ** Furthermore, these therapies may exacerbate hypotension when amyloid-associated autonomic dysfunction is present. β-Blockers and nondihydropyridine calcium channel blockers are often poorly tolerated, even at low doses, because patients with ATTR-CM rely on heart rate response to maintain cardiac output given a fixed stroke volume. 2 Kittleson MM, Maurer MS, Ambardekar AV, Bullock-Palmer RP, Chang PP, Eisen HJ, Nair AP, Nativi-Nicolau J, Ruberg FL; American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology. Cardiac Amyloidosis: Evolving Diagnosis and Management: A Scientific Statement From the American Heart Association. Circulation. 2020 Jul 7;142(1):e7-e22. doi: 10.1161/CIR.0000000000000792. Epub 2020 Jun 1. Erratum in: Circulation. 2021 Jul 6;144(1):e11. PMID: 32476490.
Other Supportive Products
Orthostatic hypotension:
- Fitted waist-high elastic stockings5
RENAL:
Anti-coagulants:
Nephrotic Syndrome:
- The presence of severe nephrotic syndrome can also increase the risk of venous thrombosis7
- Anticoagulation should be considered in patients who have other procoagulant factors, most commonly treatment with immunomodulatory drugs7
Nephrotic Syndrome:
- Albumin Infusions + Diuretics: Patients with severe nephrotic syndrome may benefit from admission for i.v. diuretics, and albumin infusions could be considered. In some patients, asymptomatic involvement of the autonomic nervous system10
- Severe Diarrhea
- Therapeutic: Loperamide1, codeine phosphate3, antimicrobial therapy3, octreotide in non-responsive cases3
- Prevent malabsorption and malnutrition3
- Oral or intravenous feeding5
- Patients who develop end-stage renal disease could initiate renal replacement therapy. However, patients with amyloidosis are prone to intradialytic hypotension due to cardiac and autonomic nervous system involvement, as well as the severe nephrotic syndrome that decreases capillary refill rates. Thus, ultrafiltration may be difficult to effectively perform. These patients may benefit from more frequent dialysis treatments to attenuate the ultrafiltration rate during each individual session7
- The median survival of patients with AL amyloidosis exceeds 3 years from dialysis initiation11,12
NERVOUS SYSTEM:
- Pharmacotherapy
- Severe Diarrhea
- See overlap with renal
- Neuropathy
- Patients with amyloidosis with neuropathy typically have small fiber involvement, which can be treated symptomatically with amitriptyline, nortriptyline, gabapentin, pregabalin, or duloxetine. Topical preparations that include various combinations of lidocaine, ketamine, and amitriptyline may also provide relief. For patients with neuropathy due to carpal tunnel syndrome, carpal tunnel release or carpal tunnel braces are of benefit.17
- Fludrocortisone and salt tablets are useful only in a few of these patients because they may aggravate congestive heart failure or peripheral edema. The a-1 receptor agonist midodrine or the anticholinergic pyridostigmine can improve neurogenic orthostatic hypotension and metoclopramide, used in diabetic gastroparesis, can help with gastric emptying17
- Carpal Tunnel Syndrome
- Surgery1
GASTROINTESTINAL:
Other Pharmacotherapy:
Constipation:
- Polycarbophil calcium1
Gastroparesis
- Prokinetic agents3 (e.g., metoclopramide)1
Severe Diarrhea
- Therapeutic: Loperamide1, codeine phosphate3, antimicrobial therapy3, octreotide in non-responsive cases3
- Prevent malabsorption and malnutrition3
Notes: *** Although GI involvement is reported in ATTRwt patients, these symptoms are less common than the ones reported in ATTRv, where GI manifestations are more frequent in early onset patients (Wixner et al. 2014).
SOFT TISSUE
- DRG Amyloidosis – Landscape & Forecast – Disease Landscape 7 Forecast Report (August 2018).
- Sanchorawala, et al. Light-Chain (AL) Amyloidosis: Diagnosis and Treatment. CJASN Nov 2006, 1 (6) 1331-1341. DOI: 10.2215/CJN.02740806.
- Mahmood, Shameem, et al. Update on treatment of light chain amyloidosis. Haematologica vol. 99,2 (2014): 209-21. DOI: 10.3324/haematol.2013.087619.
- Bokhari S, Castano A, Pozniakoff T, Deslisle S, Latif F, Maurer MS. 99mTc-Pyrophosphate Scintigraphy for Differentiating Light-Chain Cardiac Amyloidosis From the Transthyretin-Related Familial and Senile Cardiac Amyloidoses. Circ Cardiovasc Imaging 2013;6(2):195–01.
- Sanchorawala, et al. Light-Chain (AL) Amyloidosis: Diagnosis and Treatment. CJASN Nov 2006, 1 (6) 1331-1341. DOI: 10.2215/CJN.02740806.
- Falk RH. Diagnosis and management of the cardiac amyloidoses. Circulation 112: 2047–60, 2005.
- Milani, Paolo, et al. Novel Therapies in Light Chain Amyloidosis. Kidney international reports vol. 3,3 530-41. 28 Nov. 2017. DOI: 10.1016/j.ekir.2017.11.017.
- Caccialanza R, Palladini G, Cereda E, et al. Nutritional counseling improves quality of life and preserves body weight in systemic immunoglobulin light-chain (AL) amyloidosis. Nutrition. 2015;31:1228–34.
- Sica DA. Metolazone and its role in edema management. Congest Heart Fail. 2003;9:100–05.
- Bernardi L, Passino C, Porta C, et al. Widespread cardiovascular autonomic dysfunction in primary amyloidosis: does spontaneous hyperventilation have a compensatory role against postural hypotension? Heart. 2002;88:615–21.
- Pinney JH, Lachmann HJ, Bansi L, et al. Outcome in renal Al amyloidosis after chemotherapy. J Clin Oncol. 2011;29: 674–81.
- Palladini G, Hegenbart U, Milani P, et al. A staging system for renal outcome and early markers of renal response to chemotherapy in AL amyloidosis. Blood. 2014;124: 2325–32.
- Palladini G, Merlini G. What is new in diagnosis and management of light chain amyloidosis? Blood. 2016;128: 159–68.
- Vaxman I, Gertz M. Recent Advances in the Diagnosis, Risk Stratification, and Management of Systemic Light-Chain Amyloidosis. Acta Haematol 2019;141:93-06. DOI: 10.1159/000495455.
- Lin G, Dispenzieri A, Kyle R, Grogan M, Brady PA. Implantable cardioverter defibrillators in patients with cardiac amyloidosis. J Cardiovasc Electrophysiol. 2013 Jul; 24(7): 793–98.
- Sayed RH, Rogers D, Khan F, Wechalekar AD, Lachmann HJ, Fontana M, et al. A study of implanted cardiac rhythm recorders in advanced cardiac AL amyloidosis. Eur Heart J. 2015 May;36(18):1098–05.
- Dispenzieri, et al. Treatment of Immunoglobulin Light Chain Amyloidosis: Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) Consensus Statement. Mayo Clin Proc. 2015;90(8):1054-81.
- Berk JL, Keane J, Seldin DC, et al. Persistent pleural effusions in primary systemic amyloidosis: etiology and prognosis. Chest. 2003;124(3):969-77.
- Feng D, Syed IS, Martinez M, et al. Intracardiac thrombosis and anticoagulation therapy in cardiac amyloidosis. Circulation. 2009;119(18):2490-97.
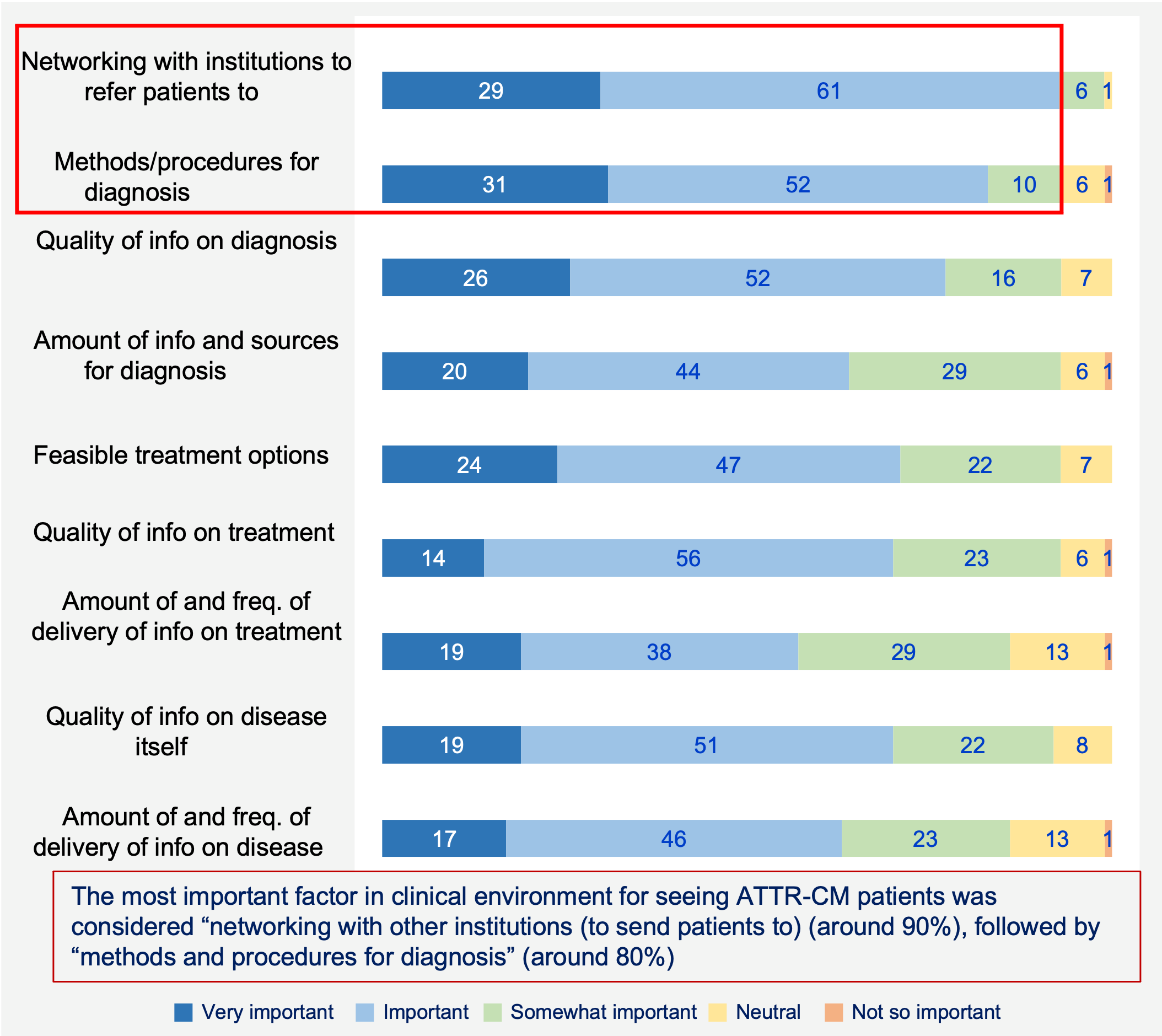
Thoughts on ATTR-CM Clinical Environment
Thoughts on clinical environment for ATTR-CM (n=90, % of total)
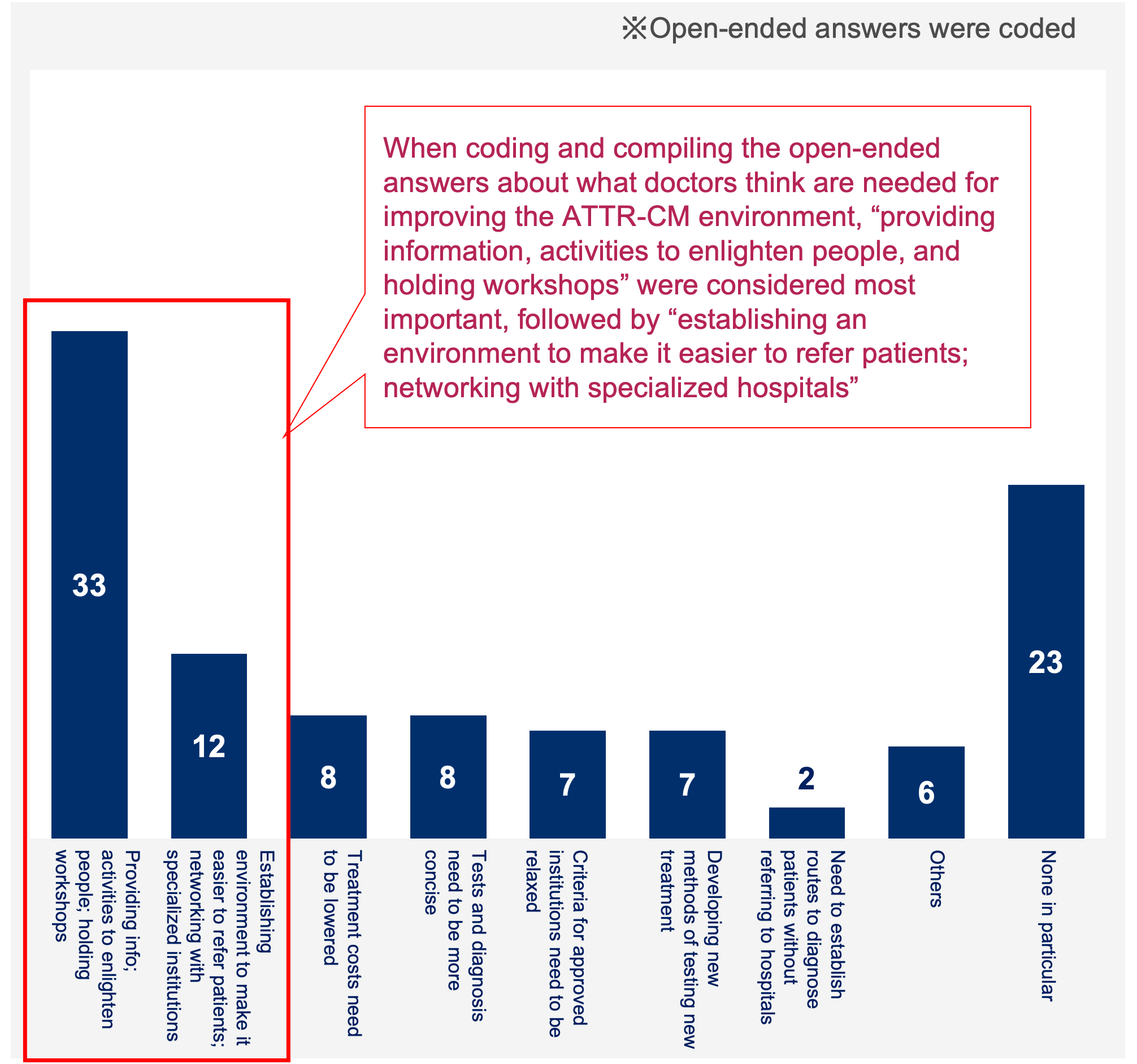
Thoughts / requests on improving ATTR-CM clinical environment (n=90, % of total)
Also, there were some cases that were referred to others for diagnostic purposes—to places that were not approved for Vyndaqel use.
On the other hand, even for “patients reaching definitive diagnosis,” research findings suggested that some of them may not have gone under the absolutely required tests—leaving room to doubt the accuracy of such diagnosis. And when it came to treatment after definitive diagnosis, application of causal therapies remained low in ratio, leaving most of such patients on symptomatic approaches on cardiac dysfunctions. These findings combined point to the possibility of certain ratios of patients left outside the proper ways of diagnosis and treatment for ATTR-CM. It is perhaps in this background that physicians’ needs (of where Vyndaqel is not approved) point to the importance of “providing more information about ATTR-CM, including those on diagnostic methods and procedures” or “networking with institutions to refer patients to,” both of which could be potential opportunities for manufacturers to participate in providing proper diagnostic methods and treatment while assisting networking for referrals.
- ALXN: Acceptance of ALXN2060 for ATTR-CM (Quantitative Survey). October 28, 2021. 02_210823_ATTR-CM quantitative research.
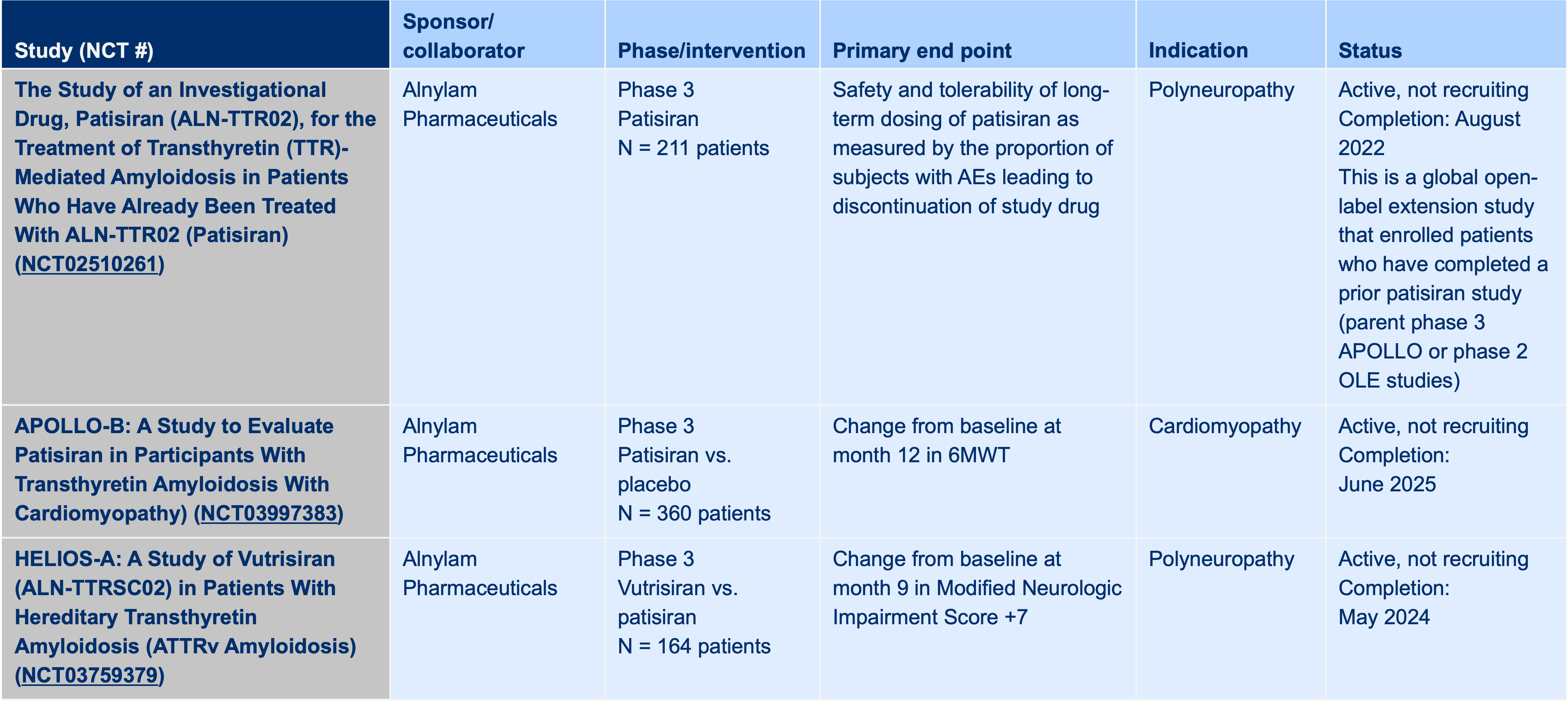
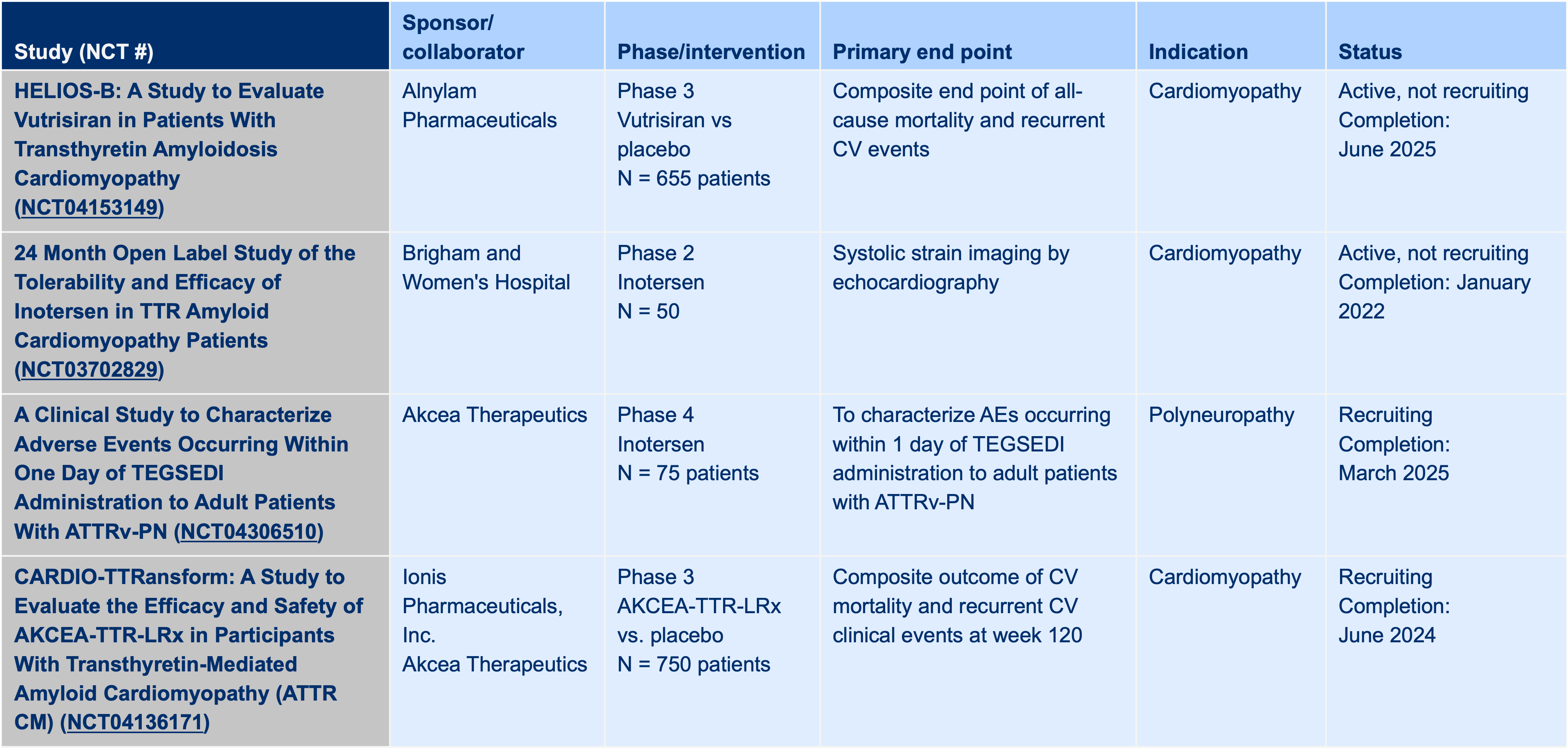
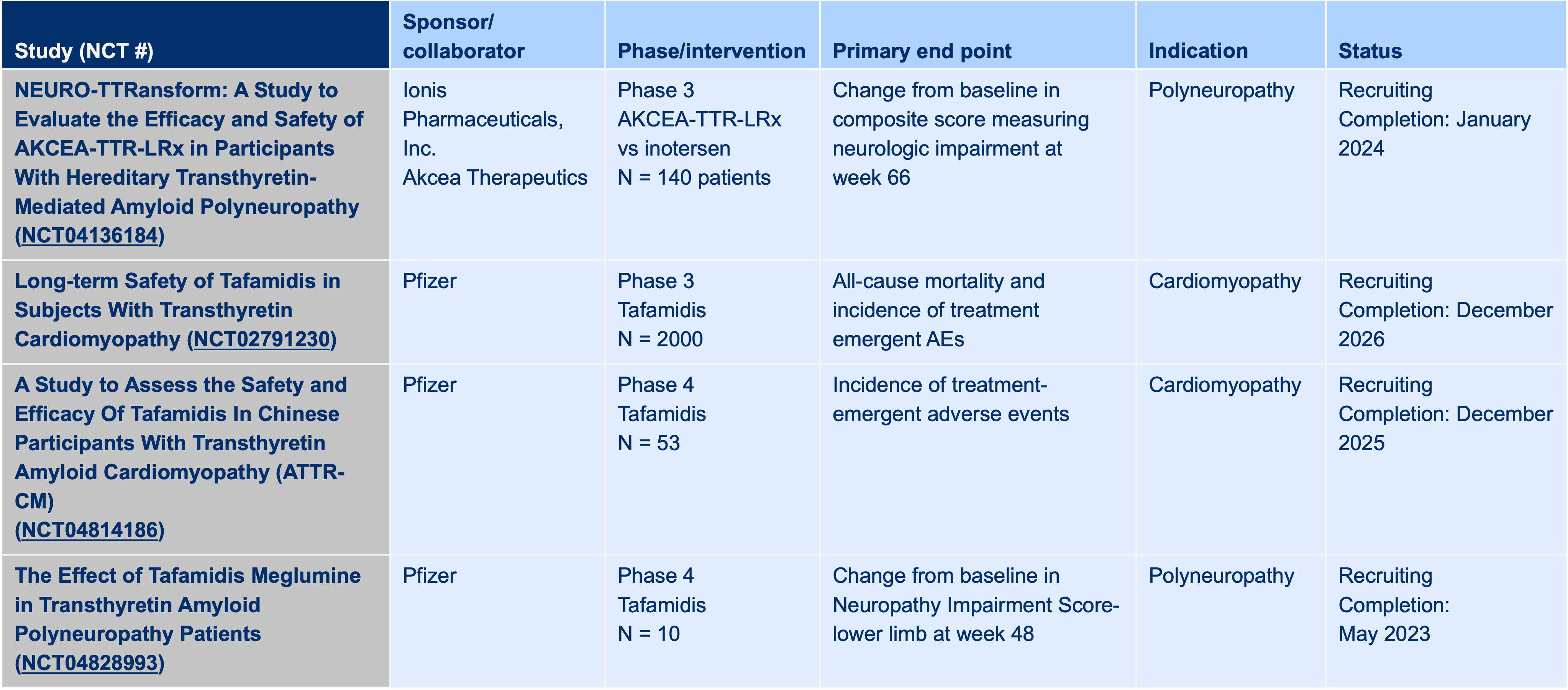
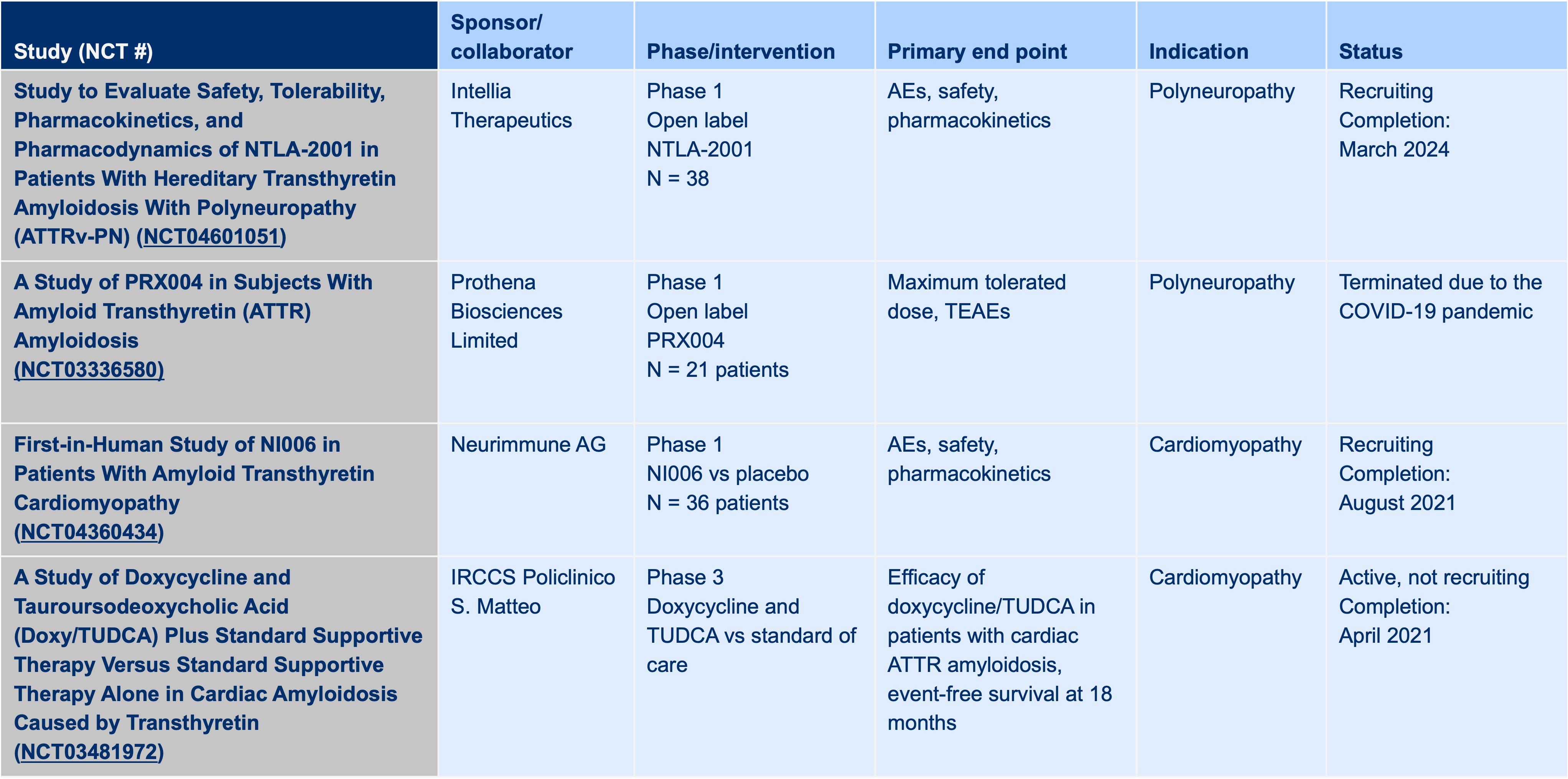
Competitor Trial Listing
- ALXN: Acoramidis for the Treatment of ATTR-CM: Training Deck. November 22, 2021.