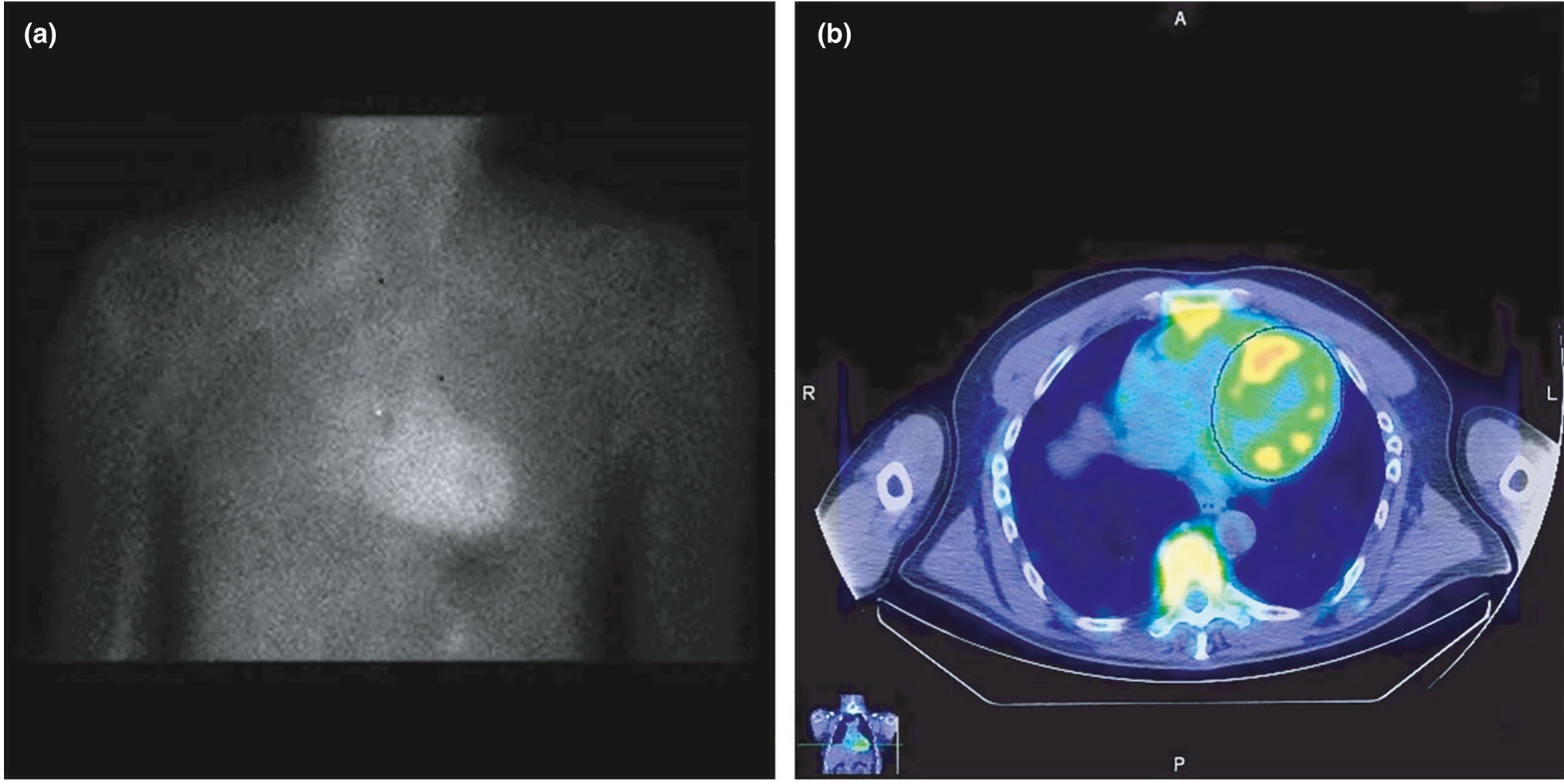
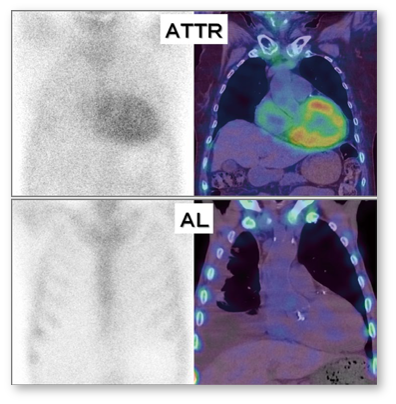
Notes: * The 99mTc phosphates currently in clinical use for cardiac amyloidosis diagnostics in Europe include 99mTc-DPD (3,3-diphosphono-1,2-propanodicarboxylate) and 99mTc-HMDP (hydroxymethylene-diphosphonate). By contrast, in the United States, 99mTc-PYP (pyrophosphate) is commonly used, while DPD is not approved. The exact mechanism that leads to the increased affinity of these radionuclides to amyloid deposits in the heart has not yet been clarified in detail but is suspected to be due to microcalcifications related to amyloid deposits. Also, the exact reason for the slightly higher affinity of these radionuclides for myocardial ATTR deposits compared to AL deposits is still unclear.2
The main advantages of scintigraphy are its relatively low costs, its established reimbursement, the wider availability compared to CMR, and the independence of image quality from patient-specific factors. However, as outlined by Kittleson et al. recently, the test performance of scintigraphy in populations with lower disease prevalence is unknown and the aforementioned positive predictive value of scintigraphy (with the absence of monoclonal gammopathy) of 100% for ATTR is questioned by some recent reports that illustrate possible causes of false-positive 99mTc-PYP scans. In addition, first larger studies with a direct comparison of scintigraphic 99mTc-DPD images with a CMR-based determination of ECV in the same patients suggest that there is a prognostic significance for the more precise CMR-based ECV. Importantly, the decision whether to perform a multi-parametric CMR study and/or a 99mTc-phosphate scintigraphy for further non-invasive work-up of suspected cardiac amyloidosis depends (amongst others) on (a) local availability and (b) respective imaging expertise.2