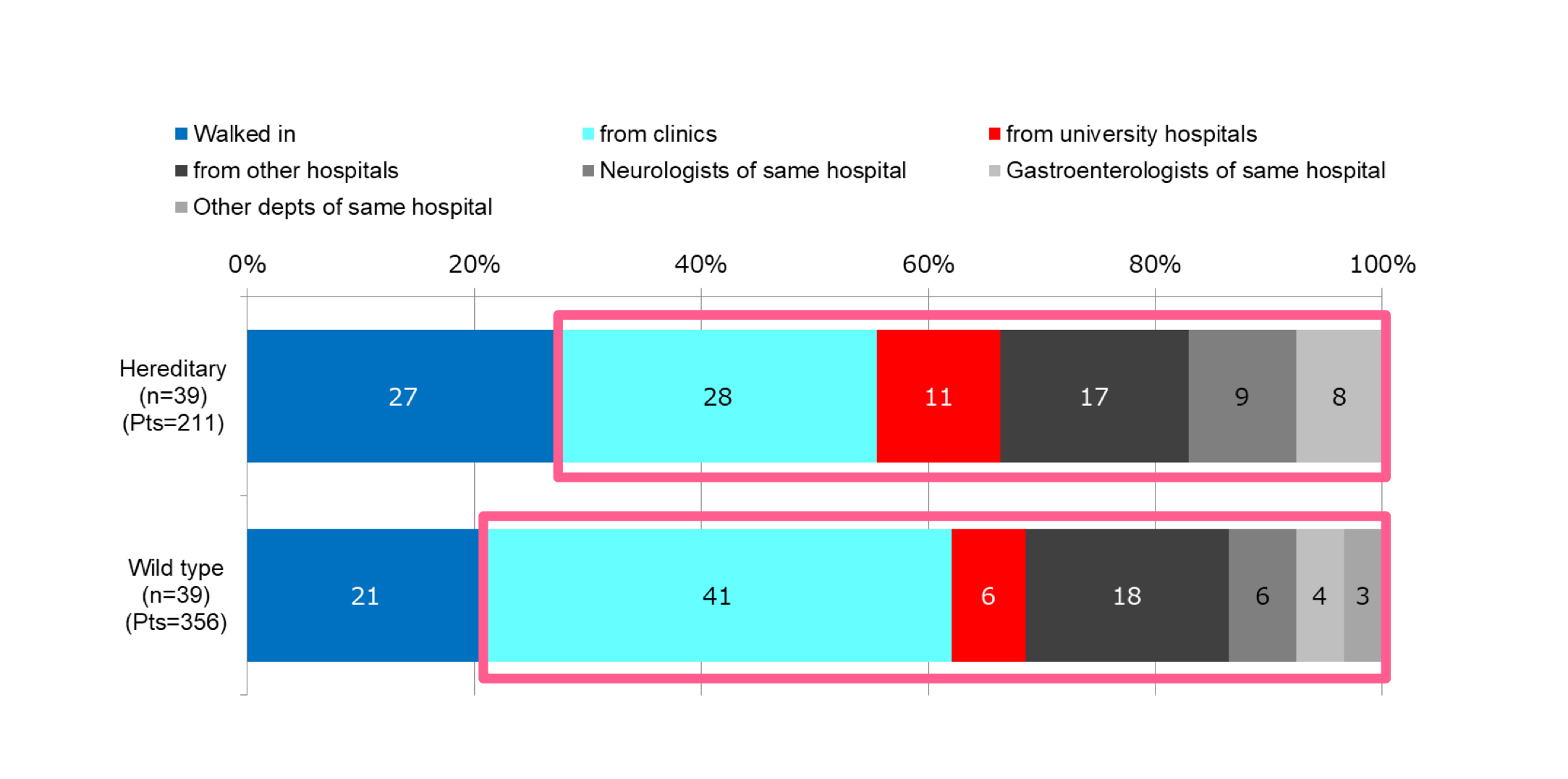
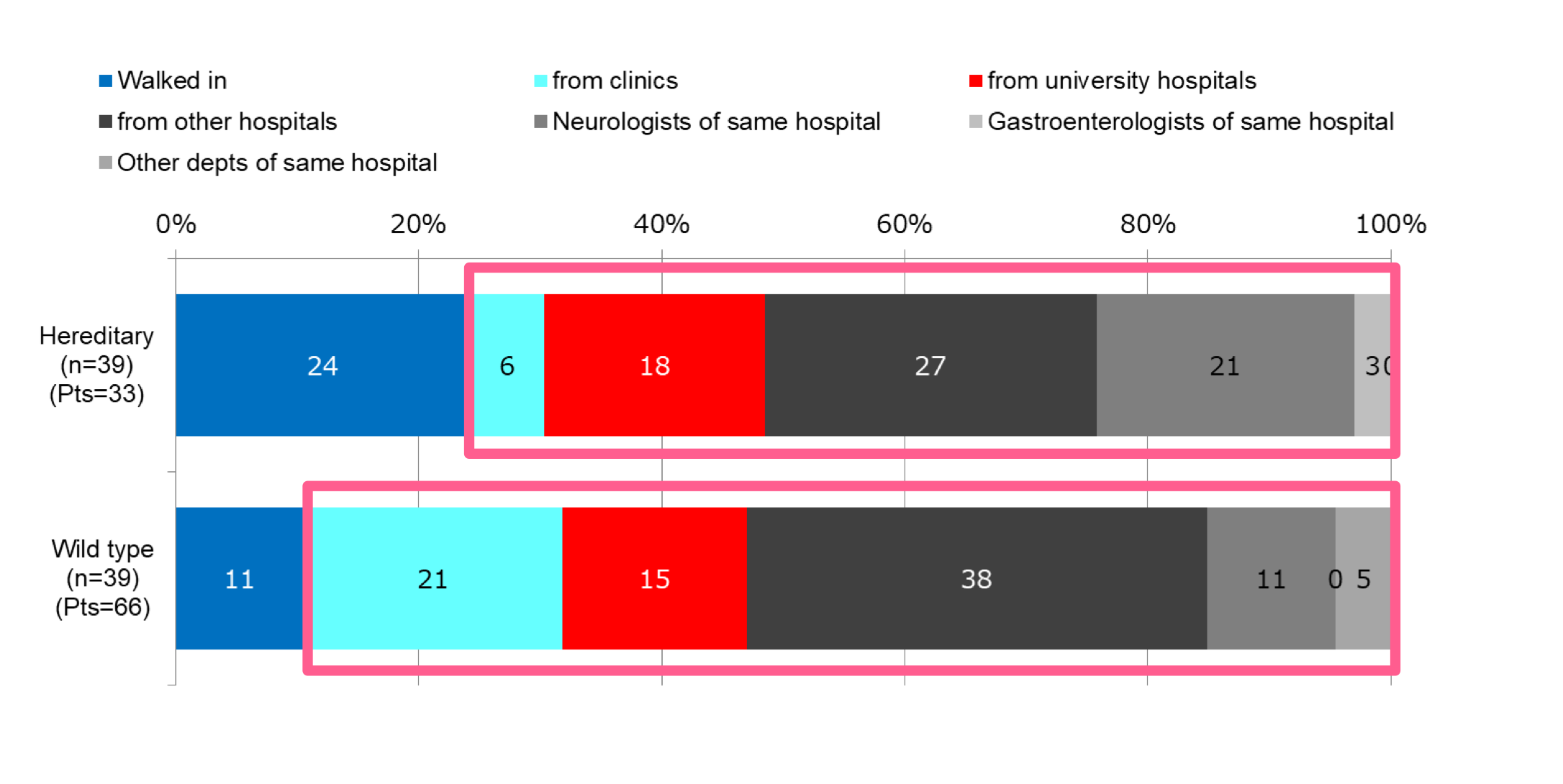
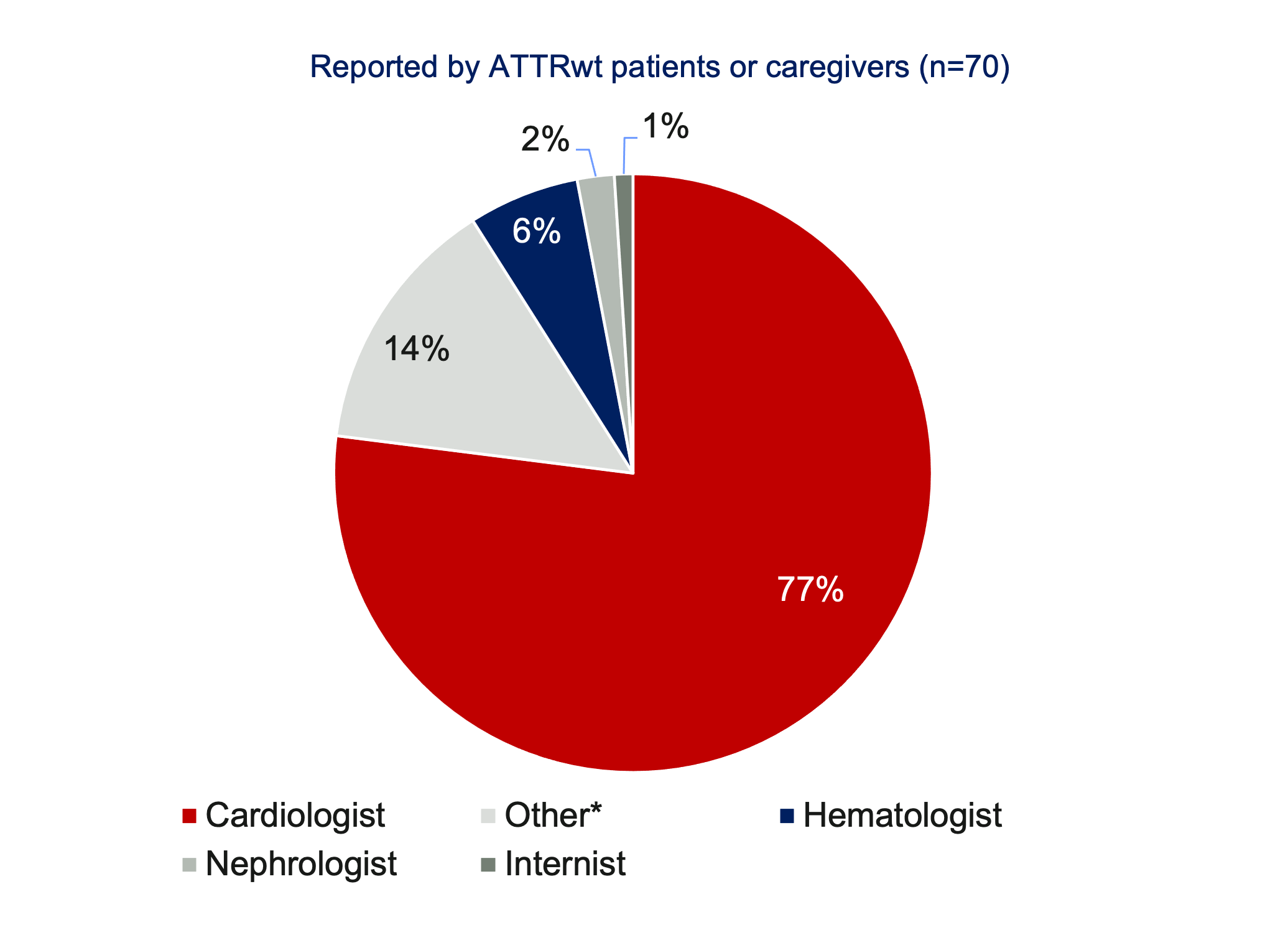
Many specialties are involved in the diagnosis of ATTR; but cardiologists are most often the diagnosing physician for ATTRwt [1,2]

Amyloidosis Survey: Results from Patients with AL and ATTR Amyloidosis and Their Caregivers. Presented at the XVIth International Symposium on Amyloidosis. 2018. Kumamoto, Japan.
Notes: Other includes internists, hepatologists, ophthalmologists & dermatologists
Notes: Surveys created by the ARC were made available on the ARC website and were given to the Amyloidosis Foundation, Amyloidosis Support Groups, and individual physicians for distribution. Of the overall total (n=699 all respondents), 54% were from the Asia-Pacific region, 17% from the EU, and 75% from North America.
- Lousada, et al. Light Chain Amyloidosis: Patient Experience Survey from the Amyloidosis Research Consortium. Adv. Ther. (2015) 32:920–28. DOI: 10.1007/s12325-015-0250-0.
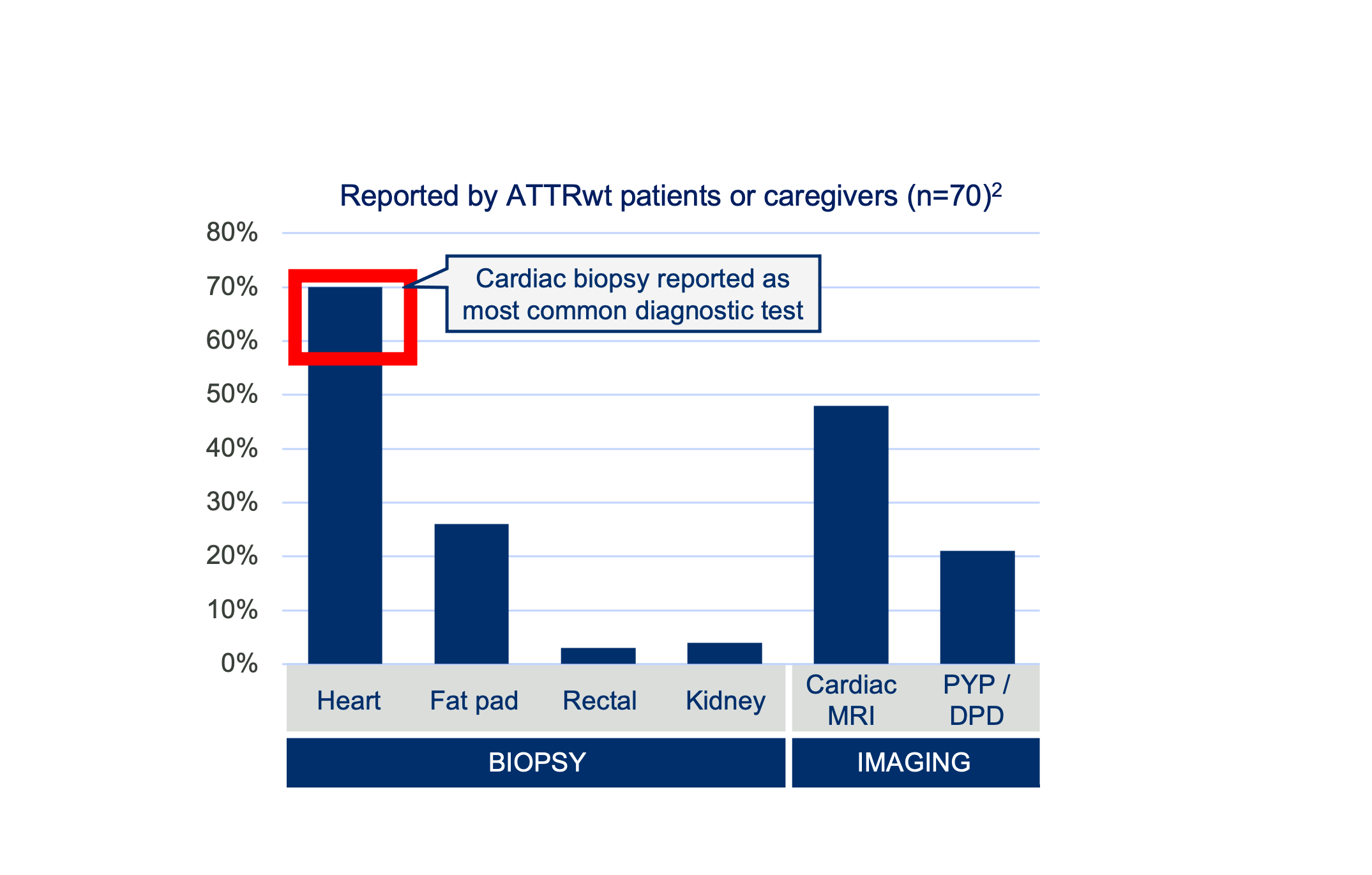
- Table 2 Establishment of amyloidosis diagnosis
- Lousada, et al. Amyloidosis Research Consortium Cardiac Amyloidosis Survey: Results from Patients with AL and ATTR Amyloidosis and Their Caregivers. Presented at the XVIth International Symposium on Amyloidosis ISA (2018) in Kumamoto.