A robust survey of US cardiologists* showed that >99% believe that patients with cardiac amyloidosis (CA) experience delays in diagnosis;
they cite misdiagnosis, low awareness of CA and diagnostic algorithm / tests as top reasons for why
they cite misdiagnosis, low awareness of CA and diagnostic algorithm / tests as top reasons for why

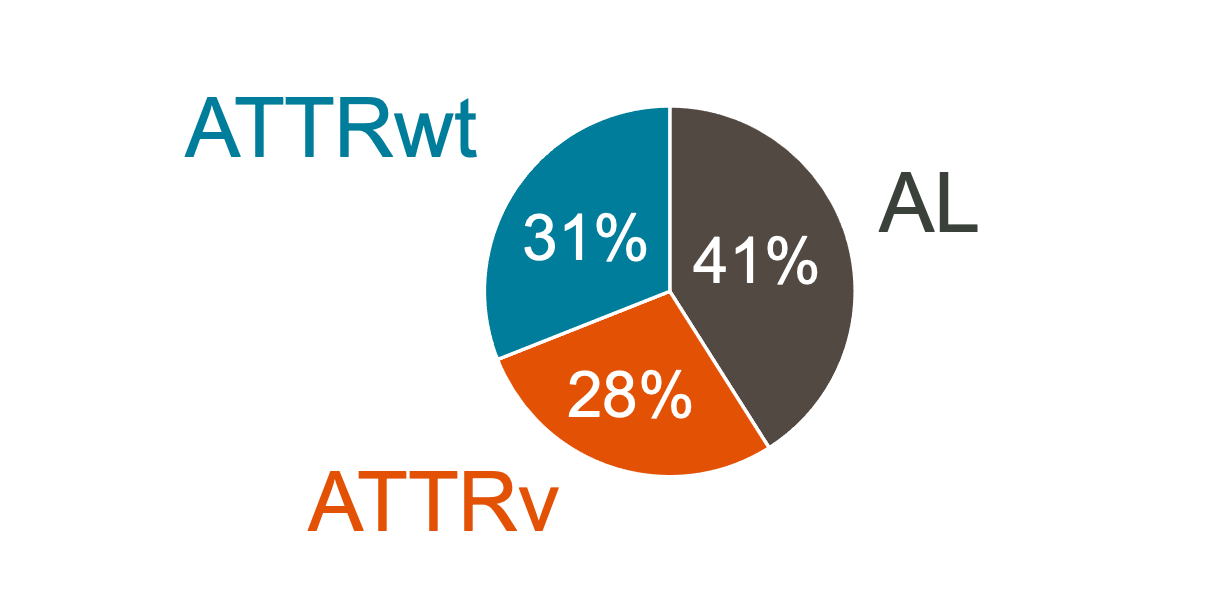
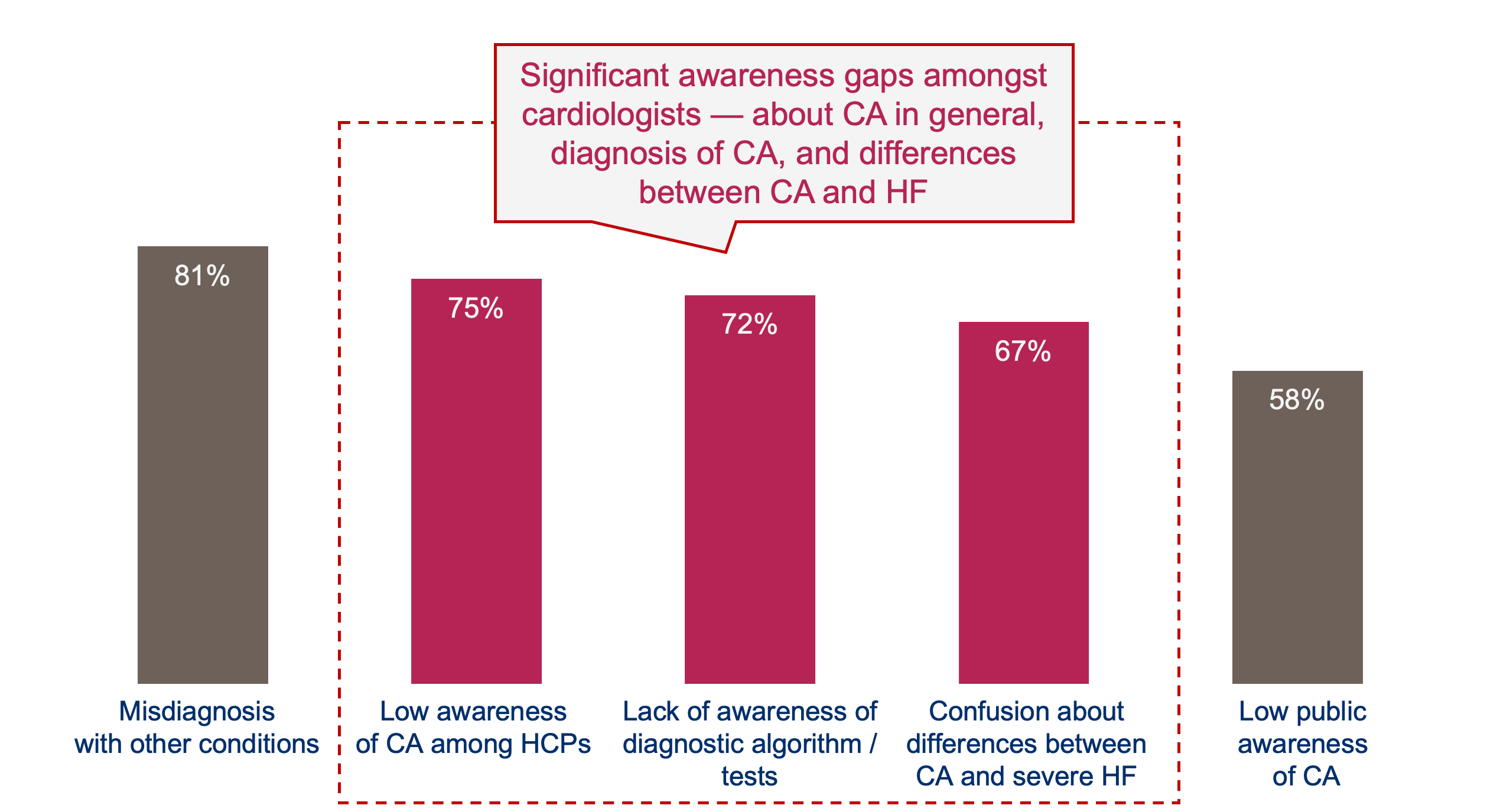
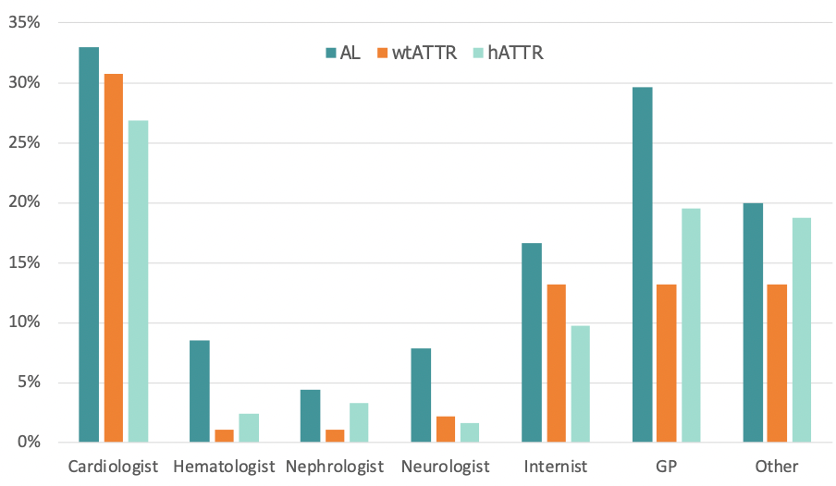
Notes: * Cardiologists (mean age 51.3 y; male, 87%; city/suburban practice, 87%; mean clinical experience, 20.2 y) saw an average of 433 patients with HF and 14.5 patients with CA in the last year. Cardiologists estimated that 41%, 28%, and 31% of their patients with CA had AL, hereditary, and wild-type disease, respectively. Nearly half of cardiologists (45%) noted an increased number of patients with CA managed in their practice compared to 5 years ago. Nearly all cardiologists (>99%) believed patients with CA experience delays in diagnosis; the most common reasons were misdiagnosis and low awareness of CA and diagnostic tests. Most cardiologists (96%) requested additional education on CA.
- Castano, et al. Cardiac Amyloidosis: Current Insights from Patients and Cardiologists Journeying Together. J. Card Fai. 2019. Vol. 25, No. 8S