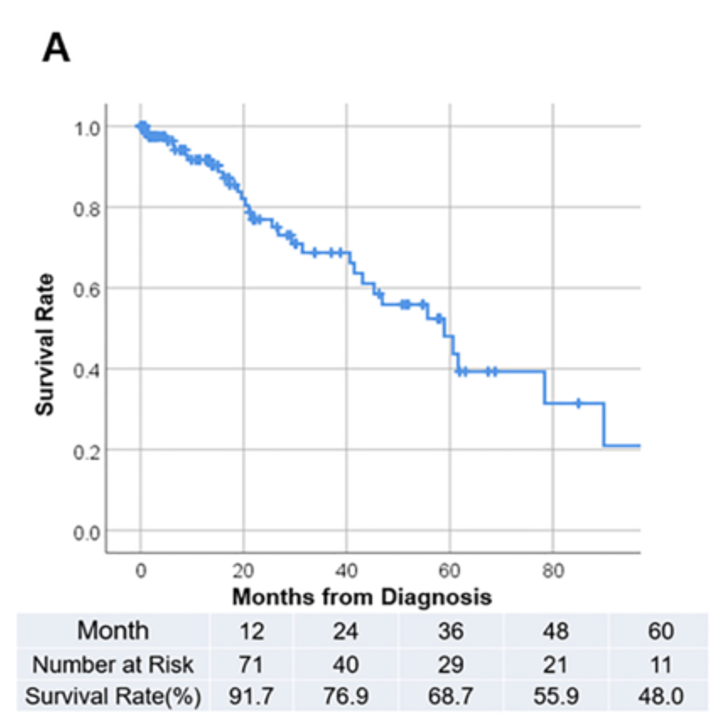
Survival studies in patients with ATTRwt-CM coalesce around median survival in the 3.5 to 5-year range; generally, ATTRv progresses even more quickly [1-7]
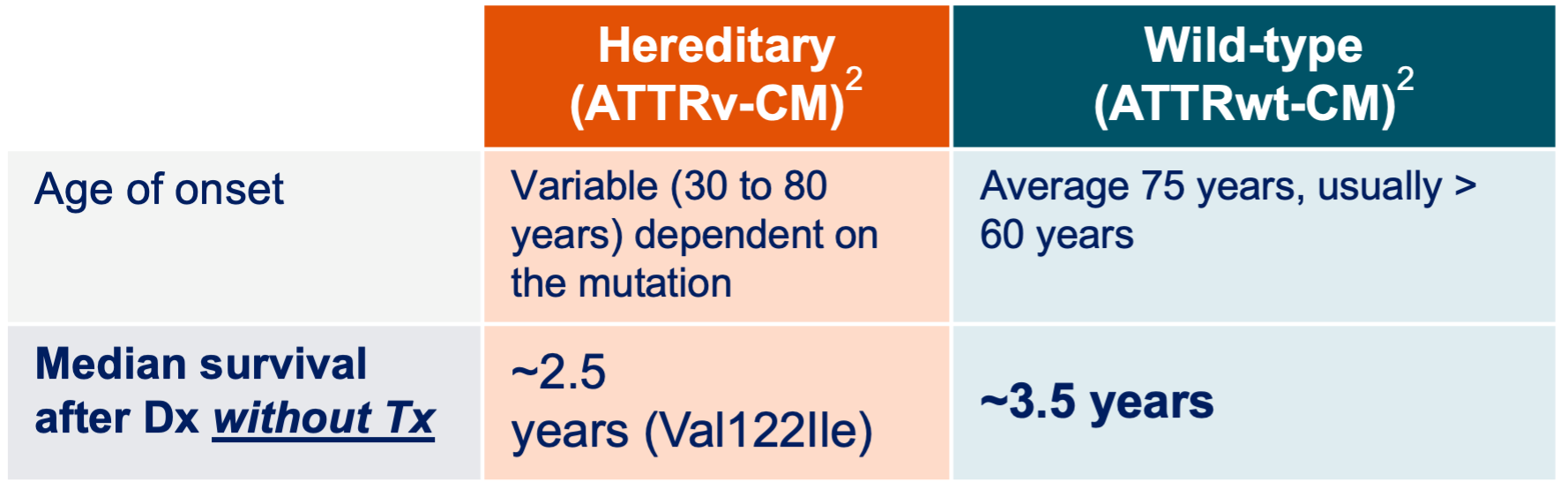
- Transthyretin Amyloid Cohort Study (TRACS): in an early longitudinal multicenter investigation that studied advanced patients, mortality with ATTR-CA was high and was worse in patients with ATTRv Val22Ile vs. ATTRwt [3]
- Common causes of death included HF, SCD, and sepsis
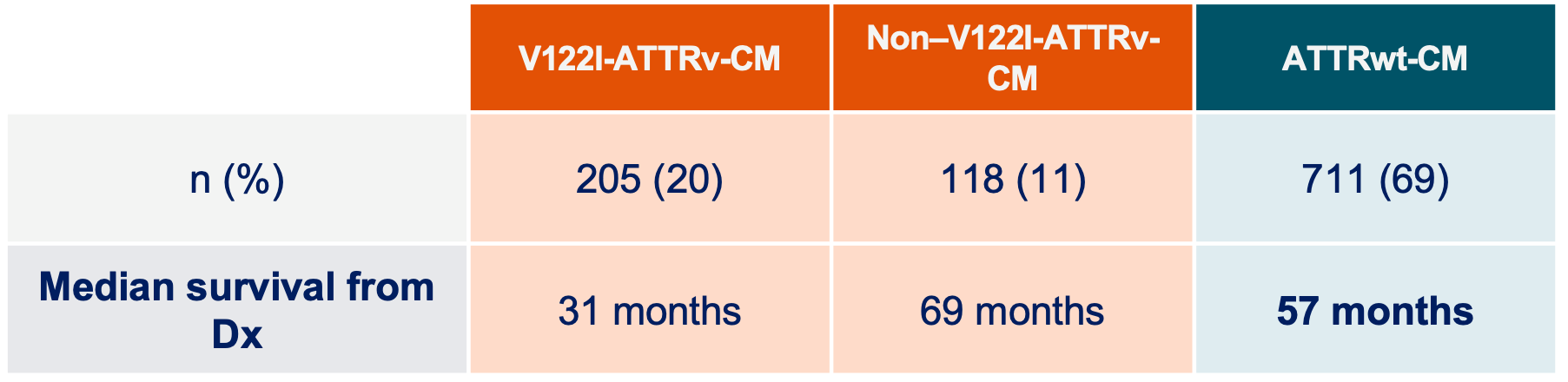
- Transthyretin Amyloid Outcome Survey (THAOS): which focused on US ATTR patients, corroborated the above data and reported significantly worse age-adjusted survival from time of enrollment over 3 years in patients with ATTRv-CA Val122Ile vs. ATTRwt-CA [3]
- A single-center US study also demonstrated significantly worse overall and age-adjusted survival from time of diagnosis in patients with ATTRv-CA Val122Ile compared with ATTRwt-CA (median survival 47 months vs. 59 months, P = .01), with survival diverging well after 24 months from diagnosis [5]
- A smaller US study also found that survival in 11 V122I ATTRv patients was worse than 18 ATTRwt patients (median survival 25.6 months vs. 43 months, respectively) [6]
Notes: CM = cardiomyopathy; HF = heart failure; SCD = sudden cardiac death
- Hendren, NS, et al. Disease-Specific Biomarkers in Transthyretin Cardiac Amyloidosis. Current Heart Failure Reports. 2020;17:77-83. https://doi.org/10.1007/s11897-020-00457-z.
- Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin Amyloid Cardiomyopathy: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;73(22):2872-2891. doi:10.1016/j.jacc.2019.04.003
- Thoracic Key: Cardiac Amyloidosis. https://thoracickey.com/cardiac-amyloidosis-4/. Accessed November 3, 2021.
- Yilmaz, A., Bauersachs, J., Bengel, F. et al. Diagnosis and treatment of cardiac amyloidosis: position statement of the German Cardiac Society (DGK). Clin Res Cardiol. 110, 479–506 (2021). https://doi.org/10.1007/s00392-020-01799-3.
- Singh A, Geller HI, Falk RH. Val122Ile mt-ATTR Has a Worse Survival Than wt-ATTR Cardiac Amyloidosis. J Am Coll Cardiol. 2017 Feb 14;69(6):757-758. doi: 10.1016/j.jacc.2016.09.987. PMID: 28183520.
- Ruberg FL, Maurer MS, Judge DP, Zeldenrust S, Skinner M, Kim AY, et al. Prospective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the Transthyretin Amyloidosis Cardiac Study (TRACS). Am Heart J. 2012;164(2):222-8 e1.
- Lane T, Fontana M, Martinez-Naharro A, Quarta CC, Whelan CJ, Petrie A, et al. Natural History, Quality of Life, and Outcome in Cardiac Transthyretin Amyloidosis. Circulation. 2019;140(1):16-26.