Both ATTRv-CM and ATTRwt-CM are associated with markedly poor QOL at the time of diagnosis, and the direction of change of QOL scores was overwhelmingly negative in all cohorts and for all domains with the fastest decline in ATTRv patients [2]
Study of ATTR-CM patients at the UK NAC between 2000 and 2017
(n = 711 patients with ATTRwt-CM, 205 with V122I-ATTRv-CM, and 118 with) non-V122I-ATTRv-CM
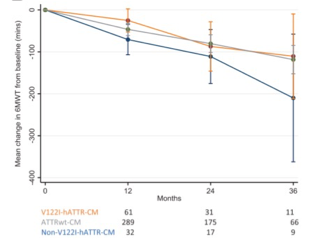
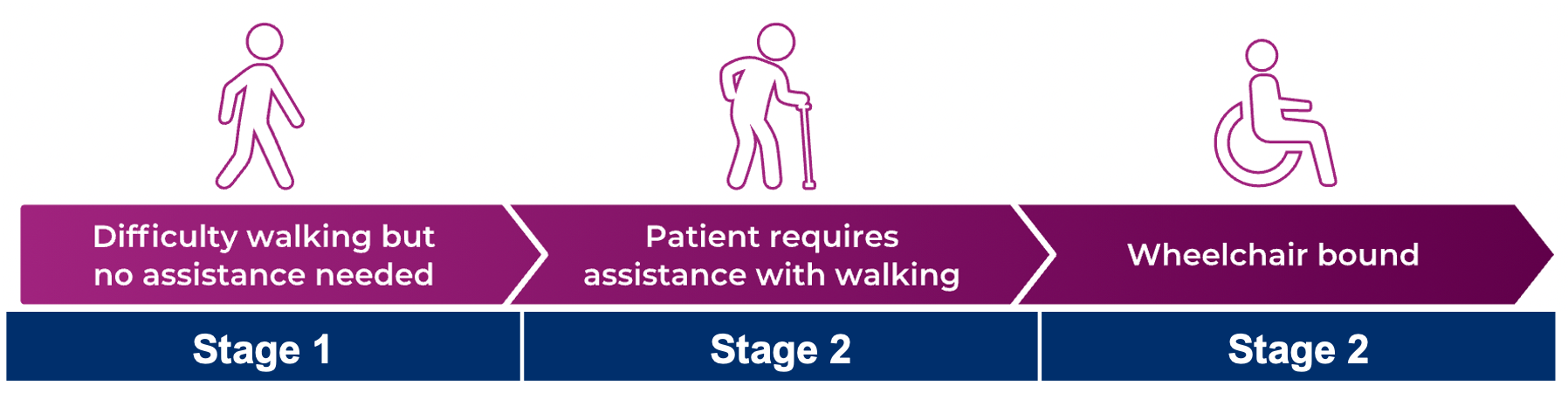
- Patients with V122I-ATTRv-CM were more impaired functionally (and had worse measures of cardiac disease at the time of diagnosis, a greater decline in QOL, and poorer survival (P<0.001) in comparison with the other subgroups
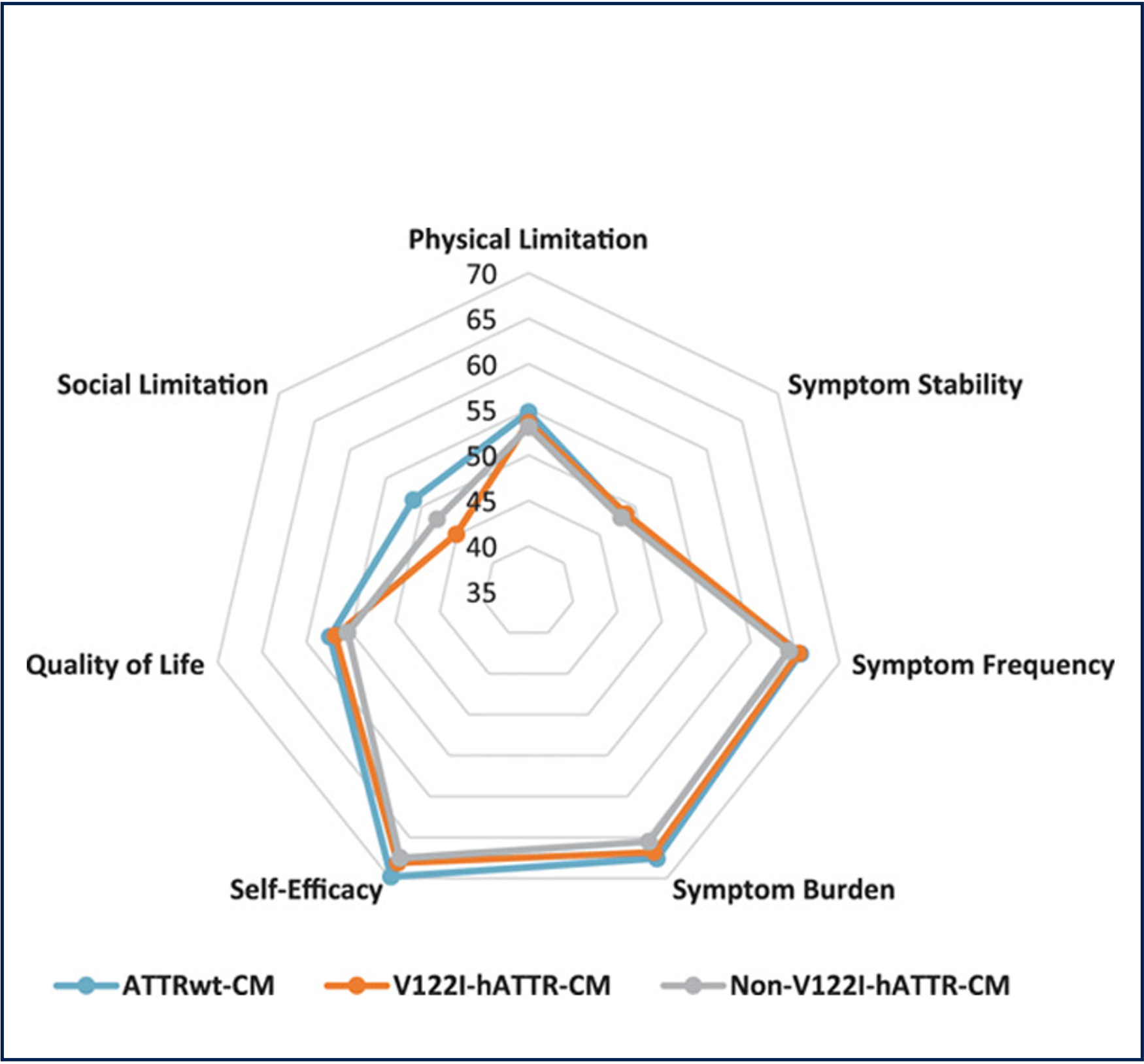
- Overall KCCQ domain scores within the first 12 months of diagnosis, obtained from 158 patients, showed poor HRQOL across all 3 genotypic subgroups of ATTR-CM
- The lowest scoring domains were physical limitation, social limitation, and symptom stability in all 3 cohorts
- The magnitude and direction of change of QOL scores in each domain were measured in each cohort between 12 and 36 months. The direction of change of QOL scores was overwhelmingly negative in all cohorts and for all domains.
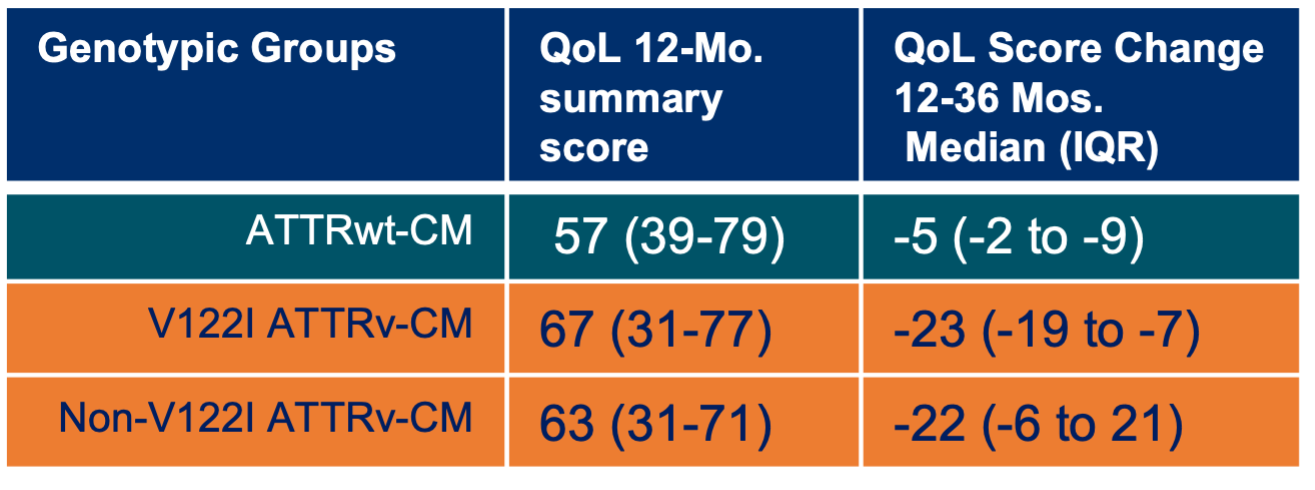
(A score of 100 indicates perfect health)
Notes: IQR = interquartile range; KCCQ = Kansas City Cardiomyopathy Questionnaire; NAC = National Amyloidosis Center; HRQOL = health related quality of life
Notes: Study of 711 patients with wild-type ATTR-CM, 205 with V122I-ATTRv-CM at the UK National Amyloidosis Center between 2000 and 2017.
- Lane, T, et al. May 21, 2019. Natural History, Quality of Life, and Outcome in Cardiac Transthyretin Amyloidosis. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.118.038169.
- ALXN: ATTR Amyloidosis: Epidemiology Dossier. Elissa Wilker & Shona Fang. September 2021. 18_ATTR Amyloidosis Epi Dossier.